
The Department of Respiratory Surgery, Tokyo Rosai Hospital
As of July 1, 2028, the Department of Pulmonary Surgery was reorganized from the Department of Surgery to a new department with two specialists. We would like to reintroduce our specialties and the diseases we treat.
Staff
| Name | Youichi Anami |
|---|---|
| Title | Director of The Department of Respiratory Surgery |
| Education | Graduated from Faculty of Medicine, Saga University in 1991 Doctor of Medicine |
| Certified physician | Japan Surgical Society |
| Medical specialist | Japan Surgical Society, Japanese Society of Pulmonary Surgery |
| Name | Takashi Makino |
|---|---|
| Title | Assistant director of The Department of Respiratory Surgery |
| Education | Graduated from Toho University in 1991 Doctor of Medicine |
| Certified physician | Board Certified Cancer Therapy Physician, Lung cancer CT screening certified physician |
| Medical specialist | Board Certified Surgeon, Japan Surgical Society, Board Certified Pulmonary Surgeon, Japanese Society of Pulmonary Surgery, Board Certified Respiratory Endoscopy Specialist, Japan Respiratory Endoscopy Association |
| Supervisor | Japanese Society of Surgery |
| Others | Councilor of the Japanese Society of Pulmonary Surgery, Clinical Training Advisor Designated physician for pediatric chronic diseases Designated physician under Article 15 of the Act on the Welfare of Persons with Disabilities (diagnosis of respiratory dysfunction) Completed the palliative care training course for doctors involved in cancer treatment, Ministry of Health, Labour and Welfare Completed the All-Japan Hospital Association training course for nurse-specific training instructors Completed the training course for program directors, Council for Clinical Training and Education |
January 1, 2022
Features
Pulmonary surgery is a department that focuses on surgical treatment of diseases of the chest other than heart and breast. In our hospital, treatment began in 2010 when I took charge of the Department of Pulmonary Surgery. The diseases covered include i) lung cancer, ii) lung cystic diseases such as pneumothorax, iii) mediastinal tumors, iv) malignant pleural mesothelioma, v) chest trauma, and vi) congenital anomalies of the lungs and bronchi, among others. The following is an explanation of the typical diseases i)-iv).
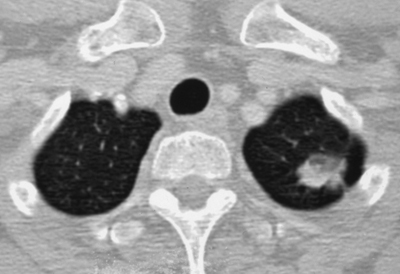
i) lung cancer
According to 2007 statistics, about 336,000 people died of cancer in Japan, and the number of deaths from lung cancer was about 66,000 (48,000 men and 18,000 women), making it the leading cause of cancer death for both men and women (24% for men and 13% for women) (1). In Japan, where smoking rates are among the highest in the industrialized world, the rate is expected to continue to increase, due in part to the aging of the population. Lung cancer symptoms often do not appear until the disease has progressed to a very advanced stage, and as a result, 40-60% of lung cancer patients are already inoperable at the time of initial diagnosis. On the other hand, with the development of CT in recent years, many small lung cancers, mainly characterized by a sliver-like shadow of 2 cm or less in diameter, have been detected in the periphery of the lung field (2). This type of lung cancer is mostly adenocarcinoma, and the 5-year survival rate after radical resection* is nearly 100%, and is considered to be equivalent to so-called early-stage lung cancer (3-6). In general, surgical resection is more curative than anticancer drugs or radiotherapy for lung cancer, so “resect while you can” is the first choice. The standard surgical procedure is **lobectomy + *** lymph node dissection. Whether or not the cancer is “resectable” is determined by the degree of progression of the lung cancer and lung function. When considering surgical treatment for lung cancer, it is important to detect lung cancer at an early stage and to treat advanced cancer appropriately in order to improve the outcome of lung cancer treatment. In other words, lung cancer treatment should be divided into early-stage lung cancer and advanced cancer.
Early-stage lung cancer
In 2010, the 7th edition of the Lung Cancer Treatment Protocol Revision (7) defined bronchioloalveolar cell carcinoma (bronchioloalveolar epithelial carcinoma) as **** an intraepithelial cancer in the lung, and proposed the concept of early-stage lung cancer for the first time. In recent years, minimally invasive surgical techniques such as thoracoscopic endoscopic surgery have been widely used to preserve pulmonary function with small wounds, and small peripheral lung cancers with mainly sliglass shadows as detected by CT are likely to be so-called non-invasive/early stage cancers based on resection results (2-6). -6), the conventional treatment of lobectomy + lymph node dissection with a large open chest is being considered instead of ***** area resection +/- lymph node dissection or partial resection only. In other words, this is a treatment that aggressively reduces the size of the wound and preserves pulmonary function. In our department, we actively perform thoracoscopic lobectomy +/- lymph node dissection in patients with small peripheral lung cancer who are eligible for such treatment.
Advanced Lung Cancer
On the other hand, anticancer drug therapy is the mainstay of treatment for advanced cancer, and multidisciplinary treatment is beginning to be used, in which anticancer drugs and radiotherapy are first used to reduce the size of the lung cancer and then resection is performed. In recent years, a number of molecular-targeted therapies, including Iressa, have been developed, and it is expected that surgery will begin to be performed after treatment with these new drugs. Thus, treatment methods have made great progress in recent years, and the indications for surgery are expanding. In addition, the use of thoracoscopes to reduce the size of the open chest wound has made it possible to perform surgery on patients with low lung function more frequently than before. The Department is actively engaged in resection of lung cancer in patients with low lung function.
As for the treatment outcome of lung cancer, the 5-year survival rate after resection of even small lung cancer without lymph node metastasis (in the case of lung cancer not mainly characterized by the aforementioned slime glass-like shadows) is different from that of early gastric cancer and remains around 80%. We speculate that the reason for this is that the outcome of treatment is inferior because the cancer is left behind due to inadequate lymph node dissection or postoperative treatment is inadequate because the cancer is misdiagnosed as “no lymph node metastasis. In our department, lung cancer resection is aggressively performed by lobectomy plus lymph node dissection using thoracotomy, and we thoroughly perform necessary and sufficient lymph node dissection to ensure that no lymph node is left behind. In the treatment of advanced lung cancer, we have a full staff of respiratory physicians, so we can provide aggressive multidisciplinary treatment combined with surgery in cooperation with the internal medicine doctors.
Thus, our department actively provides appropriate treatment according to the patient’s lung function and the degree of progression of lung cancer, whether the patient has early-stage cancer, advanced cancer, or low lung function. Please visit our hospital and our department with peace of mind.
*5-year survival rate: Percentage of treated patients who are alive 5 years after treatment.
**Lobectomy: The right lung consists of three lobes (upper, middle, and lower lobes), and the left lung consists of two lobes (upper and lower lobes). The left lung consists of two lobes, the upper and lower lobes. The lung lobe in which lung cancer exists is removed.
***Lymph node dissection: Lymph nodes are located in the fat surrounding the trachea and bronchi, and dissection means that the surrounding fat is removed from the trachea and bronchi, rather than resecting the lymph nodes alone.
**** Intraepithelial carcinoma: Cancer that has not broken through the basement membrane beneath the surface cells of the alveoli and has not invaded the alveoli. It is a cancer that remains confined to the mucosa. It is one of the so-called non-invasive cancers.
***** Zonal resection: The lung lobes are divided into smaller zones by bronchial branches. The area where the cancer is located is selectively resected. Other areas within the lung lobes are spared.
ii) Lung cystic diseases such as pneumothorax
Pneumothorax is a condition in which air leaks from the lungs due to rupture of a cyst in the lung called a bla or brevis, causing air to accumulate in the rib cage and thus crush the lung. Pneumothorax has two peak ages of onset. One group is young men around 20 years of age, and the other group is older men over 70 years of age who have continued to smoke. If the lung is collapsed in a large degree or if it occurs in both lungs at the same time, it can be life-threatening. Symptoms often include sudden chest pain and a sense of difficulty breathing, so if you have any symptoms, please seek medical attention immediately. Our hospital is well equipped to handle emergency hospitalization, so please be proactive and contact your medical provider. In addition, there is a condition called menstrual-associated pneumothorax in women, in which pneumothorax repeatedly occurs with menstruation. This disease occurs when endometrial tissue enters the chest cavity for some reason and tears the lungs as it is shed with the menstrual cycle. Treatment is by thoracoscopic surgery with a very small wound. The endometrium that has strayed into the uterus and the ruptured lung are partially resected. Afterwards, in cooperation with the obstetrician and gynecologist, hormone medication may be taken to prevent recurrence. Women who experience chest pain with menstruation are advised to visit a pulmonologist and have an x-ray when symptoms are present.
In addition, those who repeatedly suffer from pneumonia or who have prolonged fever and dirty sputum every time they catch a cold may have diseases caused by structural abnormalities of the bronchi and lungs, such as bronchiectasis or pulmonary fractionation disease. Although we have just started our practice, we are determined to build a safe and trustworthy department for our patients so that we can continue to contribute to local medical care.
iii) Mediastinal tumor
The mediastinum is a general term for a tumor that forms in the space between the left and right lungs, where the heart, large blood vessels, and trachea are located. Therefore, mediastinal tumors are difficult to detect on radiographs because they are hidden in the shadow of the heart and large blood vessels, and may be discovered with symptoms after they have grown considerably. A CT scan of the chest is necessary for diagnosis. Also, since mediastinal tumor is a general term for tumors in the mediastinum, it can be malignant or benign. Since a definitive diagnosis cannot be made until the tumor is surgically removed, surgical removal is the first choice for treatment. In the case of myasthenia gravis, even if there is no tumor, surgical removal of fatty tissue in the mediastinum is indicated because it may greatly improve the symptoms of myasthenia gravis. Generally, a longitudinal sternotomy is the procedure of choice for mediastinal tumor surgery. However, there are cases in which the possibility of a benign tumor is diagnosed as quite high before surgery by CT or MRI examination, so we perform a thoracoscopic resection with as small a wound as possible without cutting the sternum if there is a high possibility of a benign tumor.
iv) Malignant pleural mesothelioma
Malignant pleural mesothelioma is a tumor with a poor prognosis that can develop decades after exposure in patients with a history of asbestos exposure.
References
- 2005年のがん統計:国立がんセンターがん対策情報センター
- 穴見洋一:MOOK 2007~2008 肺癌の臨床:2007, p21-26, 59-64:篠原出版新社
- Noguchi M, Morikawa A, Kawasaki M, et al. Small adenocarcinoma of the lung. Histologic characteristics and prognosis. Cancer. 1995; 75: p2844‐2852
- Anami Y, Ishiyama M, Noguchi M, et al. Bronchioloalveolar carcinoma component is a more useful prognostic factor than lymph node metastasis. JTO. 2009; 4(8): p591-598
- Little AG, Gay EG, Gaspar LE, et al.: National survey of non-small cell lung cancer in the United States: epidemiology, pathology and patterns of care. Lung Cancer. 2007; 57(3): 253-60.
- Leitzmann MF, Koebnick C, Abnet CC,et al.: Prospective study of physical activity and lung cancer by histologic type in current, former, and never smokers. Am J Epidemiol. 2009 Mar 1;169(5): 542-53
- 肺癌取り扱い規約【改定第7版】:日本肺癌学会 2010年11月刊行予
Health Screening Research